Article Text

Abstract
Background: Active spondylolysis is an acquired lesion in the pars interarticularis and is a common cause of low back pain in the young athlete.
Objectives: To evaluate whether the one-legged hyperextension test can assist in the clinical detection of active spondylolysis and to determine whether magnetic resonance imaging (MRI) is equivalent to the clinical gold standard of bone scintigraphy and computed tomography in the radiological diagnosis of this condition.
Methods: A prospective cohort design was used. Young active subjects with low back pain were recruited. Outcome measures included clinical assessment (one-legged hyperextension test) and radiological investigations including bone scintigraphy (with single photon emission computed tomography (SPECT)) and MRI. Computed tomography was performed if bone scintigraphy was positive.
Results: Seventy one subjects were recruited. Fifty pars interarticulares in 39 subjects (55%) had evidence of active spondylolysis as defined by bone scintigraphy (with SPECT). Of these, 19 pars interarticulares in 14 subjects showed a fracture on computed tomography. The one-legged hyperextension test was neither sensitive nor specific for the detection of active spondylolysis. MRI revealed bone stress in 40 of the 50 pars interarticulares in which it was detected by bone scintigraphy (with SPECT), indicating reduced sensitivity in detecting bone stress compared with bone scintigraphy (p = 0.001). Conversely, MRI revealed 18 of the 19 pars interarticularis fractures detected by computed tomography, indicating concordance between imaging modalities (p = 0.345). There was a significant difference between MRI and the combination of bone scintigraphy (with SPECT)/computed tomography in the radiological visualisation of active spondylolysis (p = 0.002).
Conclusions: These results suggest that there is a high rate of active spondylolysis in active athletes with low back pain. The one-legged hyperextension test is not useful in detecting active spondylolysis and should not be relied on to exclude the diagnosis. MRI is inferior to bone scintigraphy (with SPECT)/computed tomography. Bone scintigraphy (with SPECT) should remain the first-line investigation of active athletes with low back pain followed by limited computed tomography if bone scintigraphy is positive.
- MRI, magnetic resonance imaging
- SPECT, single photon emission computed tomography
- active spondylolysis
- magnetic resonance imaging
- spondylolysis
- hyperextension
Statistics from Altmetric.com
Spondylolysis is an acquired defect in the pars interarticularis of the lumbar spine.1 It is prevalent in the general population but is often asymptomatic and detected incidentally on plain radiographs.1–3 However, it is the most common cause of persistent low back pain in young active athletes,4 where it is referred to as “active spondylolysis” in view of the symptomatic nature of the disease process.5
Active spondylolysis in young athletes has been reported in almost every sport. However, activity that involves repetitive lumbar extension and rotation such as gymnastics and diving pose a higher risk.6–8
The progression of active spondylolysis to non-union has been associated with an increased incidence of spondylolisthesis and lumbar disc degeneration.9,10 Moreover, earlier recognition of acute spondylolysis is associated with improved fracture healing11,12 and is important in preventing the formation of non-union and its consequences.
Clinical features of active spondylolysis previously described in the literature do not differentiate this condition from other causes of low back pain.3,4,13,14 In addition, there are no validated examination findings for active spondylolysis.15,16 The only reported pathognomonic finding is reproduction of pain with the performance of the one-legged hyperextension test.17,18 However, no formal study of its validity has been described.
As a consequence of the non-specific nature of clinical findings of active spondylolysis, radiological visualisation is important for diagnosis. The current gold standard investigation for young athletes with low back pain is bone scintigraphy with single photon emission computed tomography (SPECT), with the addition of limited reverse-gantry axial computed tomography if bone scintigraphy is positive (fig 1).19 There are a number of limitations in using this current diagnostic modality including the intravenous injection of radioactive tracer and the exposure of young athletes to ionising radiation.20

(A,B) Coronal and axial single photon emission computed tomography images showing bilateral increased tracer uptake at the 5th lumbar vertebra; (C) axial computed tomography image confirming bilateral stress fractures of the pars interarticularis. Permission for publication of this figure has been given.
Magnetic resonance imaging (MRI) has been shown to be as sensitive as bone scintigraphy in detecting lower limb stress fractures.21–24 It has many advantages over bone scintigraphy including the non-invasive nature of the imaging and the absence of ionising radiation.20
MRI changes in active spondylolysis include bone marrow oedema, visualised as increased signal in the pars interarticularis on oedema-sensitive sequences, and fracture, visualised as reduced signal in the pars interarticularis on T1 and T2 weighted sequences (figs 2 and 3).25–29 Although numerous studies have examined MRI changes in active spondylolysis,26–30 only one study comparing MRI with the gold standard bone scintigraphy (with SPECT)/computed tomography has been published.31 This study prospectively analysed bone scintigraphy (with SPECT), computed tomography, and MRI in a cohort of 72 young athletes with low back pain. Although good agreement was found between the imaging modalities, there were a number of limitations of the study that questioned the validity of its findings. These included lack of reliability testing of the imaging modalities and significant discordance between bone scintigraphy (with SPECT) and MRI. Clearly, there is a need to examine further the role of MRI in investigating young athletes with suspected active spondylolysis.

Reduced signal surrounded by increased bone marrow signal on a sagittal T2-weighted image: consistent with right L5 pars interarticularis stress fracture. Permission for publication of this figure has been given.

Break in cortical ring shown by reduced signal (dark line) consistent with pars interarticularis stress fracture on T2-weighted axial image. Permission for publication of this figure has been given.
The purpose of this study is to (a) evaluate the usefulness of the one-legged hyperextension test in assisting early detection of active spondylolysis and (b) evaluate the effectiveness of MRI in detecting active spondylolysis compared with bone scintigraphy (with SPECT)/computed tomography.
METHODS
Subjects
Young active subjects with a history of recent-onset low back pain were recruited. Referrals were obtained primarily from sports physicians in sports medicine clinics. The inclusion criteria of subjects included:
-
aged 10–30 years
-
engaged in regular activity
-
symptoms of low back pain for 6 months or less
-
had been assessed by a sports physician or sports medicine practitioner and a provisional diagnosis of active spondylolysis had been made
-
had been referred for bone scintigraphy (with SPECT)/computed tomography as the initial investigation.
For the purpose of this study, “regular activity” was defined as the participation in sport for leisure or competition other than activity related to daily living.
Reasons for exclusion were a contraindication to MRI and a recent history of bone scintigraphic evidence of active spondylolysis (within the preceding 12 months). As bone scintigraphic evidence of bone stress may remain for up to 12 months after diagnosis,32 excluding these subjects would eliminate those with asymptomatic bone scintigraphic changes and back pain with other causes.
Ethical approval was obtained from the University of Melbourne human research ethics committee. All subjects provided written informed consent.
Procedure
Once enrolled in the study, subjects:
-
completed a study questionnaire supervised by the main investigator relating to individual anthropometric measures and sports participation
-
had a one-legged hyperextension test performed by the main investigator
-
underwent both bone scintigraphy (with SPECT) and MRI of the lumbar spine concurrently; computed tomography was only performed if bone scintigraphy revealed changes consistent with active spondylolysis.
For bone scintigraphy, a standard dose (800 MBq) of technetium 99 methylene diphosphonate (Mallinckrodt Medical) was injected. Angiographic and soft tissue planar bone scan images were obtained about 5 s and 3 min after injection. Delayed planar and SPECT images were obtained about 3 h after injection. Images were acquired using a GE Starcom 3200i single head (rectangular) gamma camera fitted with a low-energy-resolution collimator. Projection data were acquired for 25 s per view on a 128 × 128 matrix. A total of 64 images were acquired over a 360° elliptical rotation. Tomographic reconstruction was performed on the raw data using filtered back-projection producing axial, sagittal, and coronal slices.
For computed tomography, images were performed on a GE Light Speed scanner. Images were acquired in the reverse-gantry axial plane at the area corresponding to increased radioactive tracer uptake on bone scintigraphy. Approximately six contiguous slices were acquired at each area with 3-mm slice thicknesses (table index 3 mm, 140 kV, 250–300 mA). The “effective dose” of the computed tomography was about 1 mSv per area scanned.
For lumbar spine MRI, all examinations were performed on a GE Sigma 1.5 T scanner using a phased-array spinal coil. Multisequence fast spin echo scans were obtained for all MRI examinations. The four sequences consisted of:
-
sagittal T1-weighted images (TE 14/TR 475/3.5 mm slice thickness/interslice gap 1 mm)
-
sagittal T2-weighted pre-saturated images (TE90/TR3300–4000/3.5 mm slice thickness/interslice gap 1 mm)
-
axial T2-weighted fat pre-saturated images (TE90/TR3300–4000/3.5 mm slice thickness/interslice gap 1 mm)
-
reverse-gantry oblique axial short tau inversion (STIR) images (TE 85/TR4000/3 mm slice thickness/interslice gap 1 mm).
The axial images were acquired through the lower two lumbar levels only. The acquisition matrix ranged from 256 × 192 to 512 × 256 mm.
Outcome measures
One-legged hyperextension test
The one-legged hyperextension test was performed using a protocol previously described.17 While standing, facing away from the tester, subjects were asked to stand on their left leg and raise their right leg with their right hip slightly flexed and their right knee flexed to 80°. They were asked to actively extend their lumbar spine (fig 4). The main investigator then asked if this active manoeuvre reproduced their pain. The manoeuvre was repeated on the right side by standing on the right leg.
One-legged hyperextension test. Permission for publication of this figure has been given.
The test was considered positive if it reproduced the subject’s pain.
Imaging
All imaging modalities were analysed by experienced radiologists. One radiologist analysed all MRI scans, and a different radiologist analysed the bone scintigraphy (with SPECT) and subsequent computed tomography (if performed). The analysis of the MRI scan was conducted in a separate section of the radiology building to the analysis of the bone scintigraphy and computed tomography. Therefore, each radiologist was blinded to the result of the other imaging modality.
Reporting of images for each modality was based on a grading system devised by the main investigator. Reliability studies were performed in a pilot study. For intrarater reliability, κ coefficients were 1.0 for bone scintigraphy and computed tomography and 0.87 for MRI. For inter-rater reliability, κ coefficients were 0.92 for bone scintigraphy, 0.65 for computed tomography, and 0.68 for MRI. These results show good to excellent intrarater and inter-rater reliability for the grading systems used, with bone scintigraphy showing greater consistency.
Statistical analysis
Statistics were performed using the Statistical Package for the Social Sciences (SPSS; Norusis/SPSS Inc, Chicago, Illinois, USA). A two-tailed level of significance was set at 0.05 for all tests unless otherwise specified.
Sample size calculations were based on McNemar’s test for equivalence of correlated proportions assuming that the proportion of positive MRI scans equals 0.50 with type 1 error = 0.05 and power = 0.80. These calculations were based on previous studies.23,25 At least 63 subjects were required to provide acceptable power to the study.
χ2 test of independence was used to assess the relationship between the one-legged hyperextension test and the presence of active spondylolysis as defined by the gold standard investigation of bone scintigraphy. In addition, sensitivity, specificity, negative predictive value, and positive predictive value of the one-legged hyperextension test in active spondylolysis were calculated.
McNemar’s test for equivalence of correlated proportions was used to compare the results of MRI with those of bone scintigraphy (with SPECT) and computed tomography.
RESULTS
Seventy one subjects were recruited. The most common sports associated with participating subjects were cricket (14), gymnastics (14), Australian football (11), hockey (5), and basketball (5).
Of the overall cohort, 39 (55%) had evidence of increased radioactive tracer uptake on bone scintigraphy (with SPECT) consistent with active spondylolysis. In this group, 29 (78%) were male, and all were aged 25 or below.
One-legged hyperextension test
Tables 1 and 2 give the results of the one-legged hyperextension test for each side. From these results, sensitivity, specificity, negative predictive value, and positive predictive value were calculated for each side (table 3). There was no association between the one-legged hyperextension test and the presence or absence of active spondylolysis on either side.
Analysis of the one-legged hyperextension test for the left side in 71 subjects
Analysis of the one-legged hyperextension test for the right side in 71 subjects
Analysis of the one-legged hyperextension test for each side
Imaging
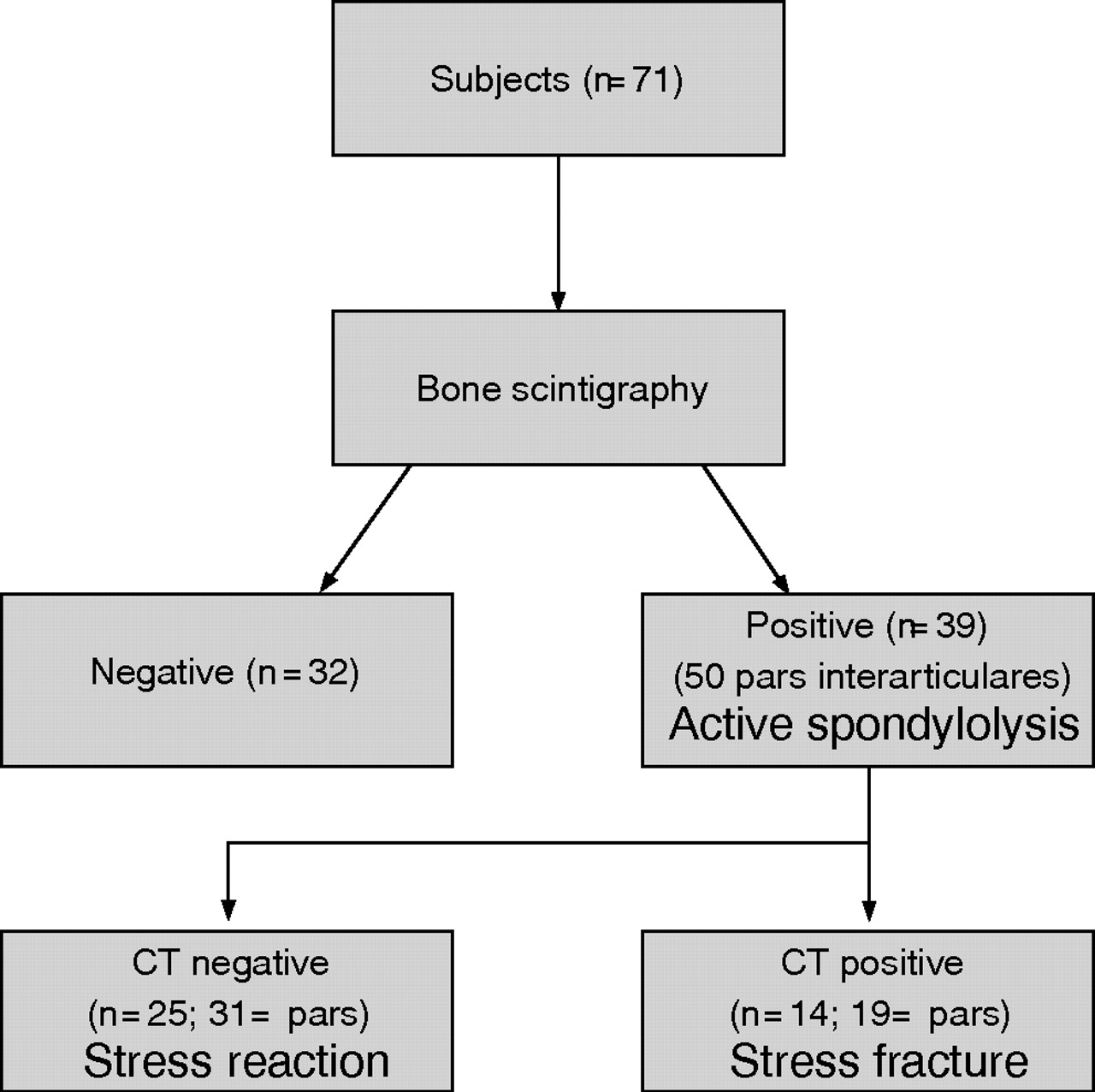
A total of 710 pars interarticulares were imaged in 71 subjects with both bone scintigraphy and MRI. Increased radioactive uptake on bone scintigraphy was detected in 39 subjects (55%). Overall, 28 subjects with positive bone scintigraphy had unilateral uptake, and the remaining 11 had bilateral uptake—that is, 50 pars interarticulares affected (fig 5).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abnormalities with bone scintigraphy (with SPECT)/computed tomography.
Of the subjects with positive bone scintigraphy, 25 (31 pars interarticulares) had a normal computed tomography, indicating stress reaction, and 14 (19 pars interarticulares) had a fracture on computed tomography, indicating a stress fracture. Most abnormalities were observed at the level of the fifth lumbar vertebra (39/50).
Comparison between bone scintigraphy and MRI
Of the 50 pars interarticulares with increased radioactive tracer detected by bone scintigraphy, only 40 (80%) were detected by MRI as bone oedema (table 4). In the 10 abnormalities not detected by MRI, seven (70%) occurred at the 5th lumbar vertebra, two (20%) at the 4th lumbar vertebra, and one (10%) at the first lumbar vertebra. There was a significant difference between bone scintigraphy and MRI (p = 0.001). These results suggest that MRI is inferior to bone scintigraphy in its ability to detect bone stress in active spondylolysis.
Comparison between bone scintigraphy (with single photon emission computed tomography (SPECT)) and magnetic resonance imaging (MRI) in detecting bone stress (n = 710)
Overall, when compared with bone scintigraphy, sensitivity, specificity, negative predictive value, and positive predictive value of MRI in detecting bone stress were 80%, 100%, 98.5%, and 100% respectively.
Comparison between computed tomography and MRI
Fifty pars interarticulares were imaged by computed tomography. Nineteen revealed evidence of a fracture. Eighteen (95%) of these fractures were detected by MRI (table 5). There was no significant difference between computed tomography and MRI (p = 0.345). These results indicate that MRI is equivalent to computed tomography in the ability to visualise fractures in the pars interarticulares.
Comparison between computed tomography (CT) and magnetic resonance imaging (MRI) in detecting pars interarticularis fractures (n = 710)
Overall, when compared with computed tomography for the visualisation of a fracture, sensitivity, specificity, negative predictive value, and positive predictive value of MRI were 94.74%, 100%, 96.88%, and 100%, respectively.
Comparison between bone scintigraphy/computed tomography and MRI
Table 6 summarises the results. There was a significant difference between changes detected on MRI and those detected on bone scintigraphy/computed tomography (p = 0.002). These results suggest that MRI is inferior to bone scintigraphy/computed tomography in its ability to detect the spectrum of changes in active spondylolysis.
Comparison between single photon emission computed tomography (SPECT)/computed tomography (CT) and magnetic resonance imaging (MRI) in detecting the spectrum of changes in active spondylolysis (n = 710)
DISCUSSION
In this study, over half of the cohort recruited was found to have active spondylolysis. This result suggests that active spondylolysis is a common cause of persistent low back pain in young active athletes. This is supported by previous research that has shown a high proportion of active spondylolysis in a similar population.4 Thus, it is imperative that doctors consider active spondylolysis as a likely cause in all young athletes with persisting low back pain.
The one-legged hyperextension test has been suggested to be pathognomonic for active spondylolysis.17 A negative test was said to effectively exclude this diagnosis negating radiological investigations.18 Examination of the one-legged hyperextension test in the present study showed that this test is neither sensitive nor specific for active spondylolysis. Moreover, its negative predictive value was poor. Therefore, a negative test cannot exclude active spondylolysis as a possible cause.
Although this is the first study to examine the usefulness of the one-legged hyperextension test in detecting active spondylolysis, this result is consistent with other studies showing lack of concordance between specific lumbar spine examination tests and lumbar spine pathology.33,34
The poor result in relation to the one-legged hyperextension test may be due to a number of factors. The test would be expected to transfer a significant extension force on to the lower lumbar spine. Although this force would place significant pressure on the pars interarticularis, it may also stress other areas of the lumbar spine such as facet joints and posterior lumbar discs, and this may subsequently cause pain in the presence of other pathology such as facet joint arthropathy and lumbar disc disease. This may explain the poor specificity of the test.
Conversely, the poor sensitivity of this test may be related to the subjective reporting of pain by subjects performing the manoeuvre, which may vary depending on individual pain tolerance. In addition, this test may preferentially load the fifth lumbar vertebra, and therefore bone stress located in the upper lumbar spine may not test positive.
The results of the one-legged hyperextension test were limited by the absence of reliability testing. Ideally, to improve the validity of this result, testing of consistency of the result should be performed.
Overall, this study suggests that the one-legged hyperextension test is a poor predictor of active spondylolysis and therefore does not assist doctors in detecting this condition. This emphasises the importance of early radiological visualisation.
What is already known on this topic
-
Active spondylolysis is a common cause of low back pain in active adolescent athletes
-
Early diagnosis improves prognosis
-
The current investigative algorithm is a SPECT scan followed by limited computed tomography if the SPECT scan is positive
-
MRI has been advocated as an alternative to SPECT/computed tomography because of proposed benefits including an absence of radiation
What this study adds
-
The one-legged hyperextension test is a poor predictor of active spondylolysis and should not be used as a diagnostic tool
-
The use of MRI as a diagnostic tool results in a significant number of false negative scans compared with the traditional SPECT/computed tomography
-
The best investigation of high-risk athletes with low back pain remains SPECT/computed tomography
The current gold standard investigation for visualisation of the spectrum of pathology in active spondylolysis is bone scintigraphy (with SPECT) with the addition of limited reverse-gantry axial computed tomography if bone scintigraphy is positive.19 MRI shows similar changes in active spondylolysis.24–28 However, there has only been one published study comparing MRI with bone scintigraphy (with SPECT)/computed tomography,31 and the conclusions of this study are questionable.
In the present study, MRI detected bone stress in 40 out of the 50 pars interarticulares in which it was detected by bone scintigraphy (with SPECT). This was significantly fewer than bone scintigraphy, which suggests that MRI is not as sensitive as bone scintigraphy (with SPECT) at detecting bone stress at the pars interarticularis. This result is discordant with other studies, which have shown similar sensitivity at other sites and at the pars interarticularis.21–24,31
There are a number of possible explanations for the discordant results in this study. The most plausible is that the inferior MRI results in this study are related to the use of a particular imaging sequence. Both sagittal and coronal MRI images used slice thicknesses and interslice gaps that were comparable to those in previous studies.25,29 However, one study26 used slightly different sequences with a slice thickness of 3 mm and an interslice gap of 0.3–0.8 mm compared with the present study which used a slice thickness of 3.5 mm and an interslice gap of 1 mm. Larger interslice gaps may reduce the proportion of bone imaged and potentially reduce the probability of detecting bone oedema—particularly in cases with subtle changes. It is possible that a reduction in interslice gap may improve the ability of MRI to detect bone stress.
Secondly, the difference in results may be related to the greater difficulty in detecting the changes of active spondylolysis by MRI. Detecting pathology by MRI relies on the interpretation of different contrasts of signals compared with normal tissue. Moreover, for active spondylolysis, this interpretation involves a small area of bone of the pars interarticularis surrounded by many other structures. Unlike stress fractures in other parts of the body, the small area of the pars interarticularis may make detection of these changes more difficult.
Conversely, in this study, 18 of the 19 fractures detected by computed tomography were also detected by MRI. There was no significant difference in the ability to detect fractures in the pars interarticularis between MRI and computed tomography. This suggests that, compared with computed tomography, MRI is able to detect fractures in active spondylolysis. Given the limitations of computed tomography, including the exposure of subjects to imaging radiation, it has been suggested that MRI may replace computed tomography for the detection of pars interarticularis fractures.
However, unlike MRI, computed tomography has the ability to differentiate between acute and chronic fractures, and this differentiation may be an important determinant of fracture healing.11,12 Therefore, although MRI may be equivalent to computed tomography in detecting fractures, its inability to determine fracture age may limit its usefulness. Accordingly, in subjects with pars interarticularis fractures detected by MRI, it may still be necessary to perform thin computed tomography slices to determine whether a fracture is acute or chronic—an important factor in fracture resolution.
The standardised grading systems used for each imaging modality in this study were found to be reliable. The blinding of the radiologists was effective, and the sample size calculations, based on expected outcome from previous studies,23,25 indicated recruitment of adequate numbers to detect statistically significant differences.
CONCLUSION
These results have implications for management of young active athletes with persistent low back pain.
-
Given the high proportion of active spondylolysis in a select population of active athletes, doctors should have a high index of suspicion and low threshold for performing early imaging of active young athletes with low back pain.
-
The one-legged hyperextension test is not useful in detecting active spondylolysis and should not be relied on to diagnose this condition.
-
Radiological visualisation is critical for diagnosis. The use of MRI as the first-line investigation may result in a significant number of false-negative scans. Despite the benefits of MRI, such as lack of radiation, we believe that, at this stage, the investigation of high-risk athletes remains with the current gold standard of bone scintigraphy (with SPECT) with the addition of thin sliced reverse-gantry axial computed tomography if bone scintigraphy is positive.
REFERENCES
Commentary
This paper addresses some crucial questions in the assessment of adolescent athletes with possible spondylolysis. The one-legged hyperextension manoeuvre, although commonly used clinically, has never been studied in this manner. It is very useful to have data on this, and it is important to recognise that there may be significant limitations in the sensitivity and specificity of this test, as there are for many other isolated provocative and subjective physical examination findings. The authors’ findings on the relative ability of MRI to identify lesions of the pars compared with SPECT and computed tomography are, perhaps, more important. There is significant disagreement among published authors on the relative utility of different imaging modalities in the diagnosis of spondylolysis. There are also very few data directly comparing the various modalities. The study of Campbell et al1 was the first to directly compare MRI with SPECT and computed tomography. This study used non-standard MRI sequences that were intended to visualise the pars optimally. Although Campbell et al concluded that MRI was “an effective and reliable first-line imaging modality” for diagnosing spondylolysis, their data actually revealed that MRI failed to identify a significant number of patients diagnosed with a stress reaction without an overt pars defect. The current study, using more standard MRI sequences (although still including one relatively non-standard sequence), showed similar results, with MRI having a reduced sensitivity for the identification of pars lesions when compared with SPECT, particularly for stress reactions without a clear fracture. From a clinical standpoint, it is extremely important to identify early stage stress fractures promptly, so that appropriate treatment can be initiated. Failing to identify these early stress reactions may lead to prolonged symptoms and, possibly, worse long-term outcomes. The current medical literature would seem to support the authors’ conclusions that bone scintigraphy with SPECT and computed tomography remain the optimal way to diagnose spondylolysis. The role of MRI and the optimal sequences for computed tomography await further study.
REFERENCE
Commentary
Many of the findings of this study are consistent with our experience in dealing with large numbers of young athletes with spondylolysis. We continue to use the hyperextension test, but interpret a posture test in the absence of pain on forward flexion as suggestive of some type of derangement of the posterior elements of the spine, including facets, etc.
Footnotes
-
Published Online First 15 September 2006
-
Competing interests: None declared.
-
Permission for publication of figures 1–4 has been given.